
From the 1Department of Clinical Gerontology, Robert-Bosch-Hospital, Stuttgart, 2Institute of Epidemiology and Medical Biometry, Ulm University, 3Center for Trauma Research, Ulm University, Ulm and 4Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Objective: Acute geriatric care (geriatric early rehabilitative treatment) and sub-acute (inpatient) geriat-ric rehabilitation are delivered to geriatric patients in Germany after hip fracture. The aim of this study was to compare patients’ outcomes after hip fracture between 3 German federal states (Hesse, Bavaria, and Baden-Wuerttemberg) that nearly exclusively offered one of the two geriatric care systems.
Design: Retrospective cohort study with patient-related health insurance claims data.
Patients: Analyses were performed with data from 2009–2012 of over 30,000 patients aged ≥80 years with incident hip fracture.
Methods: Primary outcomes: “increase in care dependency”, “nursing home admission”; secondary outcomes: “rehospitalization”, “mortality”. Multivariate regression models were applied.
Results: Compared with Hesse, the state with acute geriatric care, the risks of an “increase in care dependency” were lower in Bavaria (adjusted ratio = 0.84; 95% confidence interval (95% CI) 0.81–0.87) and Baden-Wurttemberg (0.88; 0.85–0.92), the 2 federal states with sub-acute geriatric rehabilitation. A reduction in the risk of nursing home admission was observed in Baden-Wuerttemberg (0.77; 95% CI 0.69–0.87), but not in Bavaria. Rehospitalization rates were lower in Bavaria and Baden-Wuerttemberg compared with Hesse. There was no difference in mortality.
Conclusion: Some, but not all, outcomes were more favourable in the federal states with sub-acute geriatric rehabilitation than in the federal state with acute geriatric care.
Key words: hip fracture; health services for the aged; dis-ability; care dependency; nursing home; mortality; rehabilitation; hospitalization.
Accepted Nov 7, 2019; Epublished Nov 21, 2019
J Rehabil Med 2020; 52: jrm00024
Correspondence address: Clemens Becker, Department of Clinical Gerontology, Robert-Bosch-Hospital, Auerbachstr.110, 70376 Stuttgart, Germany. E-mail: clemens.becker@rbk.de
In Germany, acute geriatric care and sub-acute geriatric rehabilitation are delivered to older patients after hip fracture. The aim of this study was to determine whether one of the two systems is superior regarding the outcomes “increase in care dependency”, “nursing home admission”, “rehospitalization” and “mortality”. Therefore, these outcomes were compared in hip fracture patients treated in 3 different federal states (Hesse, Bavaria and Baden-Wuerttemberg), which nearly exclusively offered one of the two geriatric care systems. Compared with Hesse (acute geriatric care), the risks of an “increase in care dependency” and of rehospitalization were lower in Bavaria and Baden-Wurttemberg (states with sub-acute geriatric rehabilitation) then in Hesse. A reduction in the risk of nursing home admission was observed in Baden-Wuerttemberg, but not in Bavaria. There was no difference in mortality between the 3 states. In conclusion some, but not all, outcomes were more favourable in the federal states with sub-acute geriatric rehabilitation than in the federal state with acute geriatric care.
Delivery of acute and sub-acute hip fracture care varies widely across Europe and worldwide. While standardization of surgical treatment after hip fracture has been increasingly achieved, most countries do not offer services that include orthogeriatric teams and rapid mobilization, even though advantages in terms of function and mortality have been demonstrated (1–4).
In Germany, the 16 federal states still have a major influence on how hospital care is delivered. Two-thirds of the federal states (the so-called “rehabilitation states”) offer widespread access to sub-acute inpatient geriatric rehabilitation for hip fracture patients, usually for a 3-week period in a separate rehabilitation facility (5). Until 2010, one-third of the states (the so-called “acute states”) did not often develop subacute services, due to an excessive number of acute hospital beds in these states. Instead, they offered a prolonged stay after hip fracture (and other conditions) in the acute wards. Usually the length of stay is 2–3 weeks, but it can be 4 weeks or more. The teams in both cases include physicians, nursing staff, physiotherapy, occupational therapy, and other healthcare professionals if needed. The number of therapy sessions provided in the rehabilitation clinics is higher, with 3–4 sessions per day compared with 2 sessions per day in the acute care settings.
This historical situation and practice was unchallenged until the years 2012–13, but is now increasingly under scrutiny. Since then there have been 2 developments. The “rehabilitation states” have proactively developed better acute orthogeriatric services, but have maintained the sub-acute geriatric rehabilitation services. The “acute states” were being forced by the healthcare insurers and the federal ministry of health and state governments to develop sub-acute geriatric rehabilitation services.
This was the starting point of the current healthcare service research project. The aim was to analyse the historical situation prior to the merging of the models, looking at the time period before 2012–2013. It was hypothesized that service models offering large-scale sub-acute geriatric rehabilitation after acute orthopaedic hip fracture treatment would be more beneficial to the patient. This study thereby also acknowledged the patient-reported outcome perspective that prioritizes in-home mobility and return home for home dwellers.
However, as the qualification criteria for geriatric rehabilitation have been different between the systems, direct comparison of the patient outcomes of the 2 systems may be strongly biased. To overcome this methodological problem, all hip fracture patients aged 80 years and older were included independently in the analyses if they had received any type of orthogeriatric care or geriatric rehabilitation treatment, and the outcomes were compared between those treated in “rehabilitation states” with those treated in “acute states”. The age restriction was determined a priori, since these patients are regarded as “geriatric” without necessarily having further comorbidities (6). As the first step in this analysis, 3 neighbouring federal states (Bundesländer) were pre-selected. These federal states have similar demographic and economic characteristics, such as employment rates, life expectancy, and gross income (7, 8). One state (Hesse) had politically decided to offer geriatric care almost exclusively in acute care. The other 2 states (Baden-Wuerttemberg and Bavaria) decided in the early 1990s to develop a geriatric care model almost purely in sub-acute settings (geriatric rehabilitation). The aim of this study was to use this “natural historical experiment” to perform a retrospective cohort study based on health insurance data from 3 federal states in Germany, in order to compare the effect of the 2 geriatric rehabilitation systems on different outcomes (increase in care dependency, nursing home admission, mortality, and rehospitalization) in patients with hip fracture aged 80 years or older.
Study design, data source and study participants
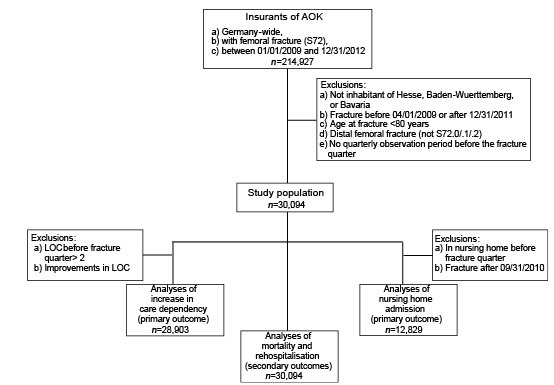
The basic dataset for this retrospective cohort study included all insured persons of the AOK (Allgemeine Ortskrankenkasse), which is the largest statutory health insurance fund in Germany, covering nearly one-third of the German population. The selection criterion was a hospital diagnosis of hip fracture between 1 January 2009 and 31 December 2012 (Fig. 1). Patient-related health insurance claims data, based on quarterly billing periods, were provided by the research institute of the AOK (Wissenschaftliches Institut der Ortskrankenkassen; WIdO). Data included information on patients’ sex, month and year of birth, level of care and nursing home status per quarterly period, date of admission to and discharge from hospital with corresponding diagnoses and performed medical measures, anonymized hospital identification number and, if applicable, admission to inpatient rehabilitation after hospital stay, information about death per quarterly period and end date of insurance. The quarterly period Q1 (e.g. 1 January – 31 March) before the quarter in which the hip fracture occurred (e.g. 1 April – 30 June) was used to derive baseline characteristics (e.g. level of care and nursing home status before fracture). Data between 1 April 2009 and 31 December 2011 were used to identify patients with hip fractures. Adequate follow-up time, which differs between the outcomes (see later definition of outcomes), was guaranteed for each patient by using the year 2012 as follow-up period. Because the exact date of the fractures was not available, the date of admission to the hospital due to the fracture was taken as the date of the fracture. This hospital stay was defined as index hospital stay (IHS). The study was approved by the ethics committee of Ulm University (application number 178/15).
Fig. 1. Study population for analyses. AOK: Allgemeine Ortskrankenkasse, a health insurance company in Germany; n: number of participants. LOC: level of care.
Care dependency expressed as level of care needs (Pflegestufe)
In Germany, it is compulsory to have long-term care insurance as well as health insurance. Long-term care insurance was introduced in the German social insurance system in 1995. From 1995 to 2016 the individual need for long-term care was categorized into 3 levels and assessed by a nurse or physician of the medical service of the German statutory health insurance system (9). This classification showed good inter-rater reliability and can be utilized as a reliable measure for the degree of mobility disability, functional impairment and, to a lesser degree, of cognitive impairment (9). The first level of care (level 1) requires a mean care need of at least 90 min per day containing more than 45 min of basic activities of daily living (ADLs). Levels 2 and 3 require a mean care need of at least 180 and 300 min containing more than 120 and 240 min of basic ADLs, respectively, per day.
Inclusion and exclusion criteria
All insured patients living in Hesse, Bavaria and Baden-Wuerttemberg, aged 80 years or older, with a hip fracture within the identification period and at least one-quarter observation time before the fracture were included. Hip fractures were identified using the hospital diagnoses coded as ICD-10 S72.0-S72.2 (n = 30,094). For the analysis of the outcome “increase in care dependency”, patients with baseline level of care (LOC) > 2 were excluded, because further worsening was not possible (ceiling effects), and patients with improvements in LOC due to low numbers and implausibility (n = 39), resulting in a dataset of 28,903 hip fracture patients. For analysis of the outcome “nursing home admission”, patients already living in a nursing home before the quarter in which the fracture occurred, and, due to problems with the validity of the nursing home information, fractures after the 31 September 2010 were excluded, resulting in a dataset of 12,829 patients with hip fracture.
Definition of covariates
Age at date of fracture was used as a continuous variable. The Elixhauser comorbidity score measures comorbidity based on additional diagnoses during the IHS and is expressed in score points (10, 11). Level of care Q1 was a categorical variable with categories “no care need”, “level 1”, “level 2” and “level 3” measured in the quarterly period before hospital admission, representing the degree of care dependency before fracture.
Definition of exposure: rehabilitation systems acute vs sub-acute treatment
There are 2 different systems of geriatric rehabilitation offered in different federal states in Germany:
1) Rehabilitation during acute hospital stay and its reimbursement as part of the acute treatment (§108/109: so-called “geriatric early rehabilitative treatment”). Geriatric early rehabilitative treatment was retrieved from the hospital data by the unique OPS (Operationen- und Prozedurenschlüssel) code: 8–550. The German procedure classification (OPS) is the official classification for the coding of operations, procedures and general medical measures in the inpatient sector (12). The procedure 8–550 stands for a complex rehabilitative treatment by a multidisciplinary geriatric team for at least 14 days and is headed by a geriatrician. In patients with hip fracture, this multidisciplinary geriatric treatment begins usually early after surgery (e. g. commencing first physiotherapeutic mobilization within 24 h after surgery) (5). During the study period, the complex rehabilitative treatment (OPS8-550) was usually delivered in a geriatric unit. In Hesse, this type of rehabilitation during acute hospital stay was nearly exclusively offered during the study period (“acute state”).
2) Sub-acute geriatric rehabilitation is delivered in a geriatric rehabilitation unit after discharge from acute care (§111: “Inpatient geriatric rehabilitation”) and usually has a duration of 3 weeks, with the option to extend rehabilitation if needed. Patients receive therapy by a multidisciplinary geriatric team headed by a geriatrician. During the study period, geriatric treatment in Bavaria and Baden-Wuerttemberg was nearly exclusively offered as sub-acute geriatric rehabilitation (“rehabilitation states”). However, routine health claims data did not directly allow discrimination of sub-acute geriatric rehabilitation from sub-acute orthopedic rehabilitation. Therefore, the daily cost of the rehabilitation as a surrogate measure was used to discriminate the 2 different types of rehabilitation. Geriatric rehabilitation was identified if the daily rate was higher than 142.9 Euros; otherwise ortho-paedic rehabilitation was assumed. Only rehabilitation stays starting within 28 days after discharge from IHS and only the first rehabilitation stay within 6 months after the fracture were considered. Directly consecutive rehabilitation stays were combined.
Definition of outcome variables
For the 2 primary outcome variables “increase in care dependency” and “nursing home admission”, the information was available on a quarterly period basis only. The increase in care dependency was defined as a new onset of care need (i.e. new classification in 1 of the care levels after fracture) or a higher care level in the quarterly period after the fracture compared with the quarterly period before the fracture. The alternative post-fracture outcome state was no change in care dependency (i.e. no classification in one of the care levels after fracture or an identical care level pre- and post-fracture). A nursing home admission was detected when the patient was not in a nursing home in the quarterly period before the fracture, but was institutionalized in the quarterly period after the fracture. Due to the information structure being on a quarterly period basis, it was not possible to determine whether an “increase in care dependency”, or admission to a nursing home, which occurred in the same quarterly period as the hip fracture, happened before or after the injury.
Secondary outcome variables were mortality and rehospitalization. Mortality was assessed by month and year of death. The occurrence and duration of any rehospitalization were detected by data on inpatient hospital stays for any reason. The outcome variables mortality and rehospitalization were identified within a period of 26 weeks (6 months) after hip fracture.
Statistical analysis
Baseline characteristics were described by means and standard deviations or numbers and percentages, stratified for the 3 German states Hesse, Bavaria and Baden-Wuerttemberg. The transition probabilities represent the rates of “increase in care dependency” or rates of nursing home admission after standardization for age and sex (in %). The rates of mortality and rehospitalization were also standardized for age and sex. The standardization was based on the total German population of all hip fracture patients (hospital discharge diagnosis S72.0–S72.2) aged 80 years and older (www.destatis.de).
Log-binomial regression models were calculated to estimate the relative ratios of “increase in care dependency” and of admission to nursing home in the quarterly period after hip fracture. In these models, death before the end of the observation period was treated as a competing event. Log-Poisson-regression models were applied to estimate rate ratios of mortality and of rehospitalization within 26 weeks after hip fracture. Follow-up time was considered as the time-varying variable, with one observation per person-day under risk, in order to avoid comparisons in times where no event is possible. Time since fracture was included as spline term in order to allow the rates to change non-linearly over time, while assuming proportionality between groups. In the analyses of rehospitalization only comparisons between persons already discharged from IHS were performed (left truncation). In Fig. S11, the age- and sex-adjusted rates per 1,000 person weeks were shown with splines for each federal state, including a time-state-interaction term in the model calculation, thereby relaxing the proportionality assumption of previous models. For the cumulative mortality, the daily mortality rates were accumulated while accounting for right censoring.
All models were enlarged stepwise with adjustment for age and sex, Elixhauser comorbidity score, and level of care Q1. p-values less than 0.05 were used to detect exploratory statistical significance. All calculations were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA) and R, version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria). The study was approved by the ethics committee of Ulm University (application number 178/15).
The mean age, sex distribution and Elixhauser comorbidity score were similar in the 3 federal states (Table I). However, statistically significant differences could be observed regarding level of care and nursing home status in the quarterly period before the fracture. A complete geriatric early rehabilitative treatment (OPS 8–550) during acute geriatric care was delivered to nearly half of all patients in Hesse, whilst the same procedure was only very seldom (Bavaria: 2.9%) or seldom (Baden-Wuerttemberg: 8.3%) delivered in the 2 federal states with mainly sub-acute geriatric rehabilitation. In contrast, hip fracture patients in Bavaria and Baden-Wuerttemberg more frequently received any rehabilitation (53.8% and 49.4%) or geriatric rehabilitation (30.4% and 36.7%) than hip fracture patients in Hesse (1.9% with sub-acute geriatric rehabilitation). The difference in the type of care is reflected in the different lengths of stay. At the IHS the mean length of stay was considerably higher in Hesse (25.4 days), the federal state with acute geriatric care, than in Bavaria (16.6 days) and Baden-Wuerttemberg (16.7 days), the 2 federal states with a very limited availability of acute geriatric care. However, the combined mean length of stay of the (acute) IHS and the (sub-acute) rehabilitation was similar in the 3 federal states (approximately 28 days).
Primary and secondary outcomes in hip fracture patients from Bavaria and Baden-Wuerttemberg were compared with the outcomes in hip fracture patients from Hesse. The results are presented in Fig. 2 and Table II. Age- and sex-standardized transition probabilities for an increase in care dependency were 40% for patients in Hesse and 36% and 37% for patients in Bavaria and Baden-Wuerttemberg, and were statistically significant as the confidence intervals of the point estimates were not overlapping. The adjusted relative risk of an increase in care dependency after hip fracture was 16% (95% confidence interval (95% CI) 13–19%) lower in Bavaria and 12% (95% CI 8–15%) lower in Baden-Wuerttemberg than in Hesse. A reduction in the rate of nursing home admission was observed in Baden-Wuerttemberg (adjusted ratio 0.77, 95% CI 0.69–0.87), but not in Bavaria. There was no statistically significant difference in the adjusted 6-month mortality between the 3 federal states (Figs S1–S31). Finally, hospital readmissions were lower in Bavaria and Baden-Wuerttemberg, the 2 federal states with sub-acute geriatric rehabilitation, than in Hesse, the federal state with acute geriatric care.
Table I. Characteristics of patients with hip fracture at hospital admission in the German federal states Hesse, Bavaria and Baden-Wuerttemberg
Primary and secondary outcomes in hip fracture patients from Bavaria and Baden-Wuerttemberg were compared with the outcomes in hip fracture patients from Hesse. The results are presented in Fig. 2 and Table II. Age- and sex-standardized transition probabilities for an increase in care dependency were 40% for patients in Hesse and 36% and 37% for patients in Bavaria and Baden-Wuerttemberg, and were statistically significant as the confidence intervals of the point estimates were not overlapping. The adjusted relative risk of an increase in care dependency after hip fracture was 16% (95% confidence interval (95% CI) 13–19%) lower in Bavaria and 12% (95% CI 8–15%) lower in Baden-Wuerttemberg than in Hesse. A reduction in the rate of nursing home admission was observed in Baden-Wuerttemberg (adjusted ratio 0.77, 95% CI 0.69–0.87), but not in Bavaria. There was no statistically significant difference in the adjusted 6-month mortality between the 3 federal states (Figs S1–S31). Finally, hospital readmissions were lower in Bavaria and Baden-Wuerttemberg, the 2 federal states with sub-acute geriatric rehabilitation, than in Hesse, the federal state with acute geriatric care.
Fig. 2. Age- and sex-standardized transition probabilities (%, point estimates with 95% confidence intervals) for primary outcomes “Increase in care dependency” (left panel) and “Nursing home admission” (right panel) after hip fracture in the German federal states Hesse (HE), Bavaria (BY) and Baden-Wuerttemberg (BW).
Table II. Comparison of outcome parameters after hip fracture between the 3 German federal states Hesse (reference), Bavaria and Baden-Wuerttemberg
A German natural historical experiment was used to compare the outcomes of 2 geriatric rehabilitation systems on different outcomes in patients with hip fracture. The 2 federal states that offered sub-acute geriatric rehabilitation had lower rates of an increase in care dependency and of rehospitalization. The effect of the treatment system on nursing home admission was inconsistent. In the state offering the highest number of sub-acute geriatric rehabilitation episodes (Baden-Wuerttemberg) nursing home admission was lower compared with the other scenarios. No difference in 180-day mortality was observed between the compared care systems.
Abbas et al. evaluated the same scientific question, but chose a different methodological approach (13). They used data from the year 2007 from the same data source as our study and compared different outcomes of patients with hip fracture who received either geriatric early rehabilitative treatment (OPS 8–550 procedure) during acute geriatric care or sub-acute geriatric rehabilitation. They did not find differences in rehospitalization rates and mortality between patients of 1 of the 2 geriatric treatment systems. Our approach, however, included not only patients who actually received 1 of the 2 geriatric types of treatment, but all patients who should have been treated by geriatricians. Therefore, we included, on the one hand, all AOK-insured hip fracture patients from a federal state (complete coverage), but on the other hand restricted the dataset to patients aged 80 years and older, since this age group is considered “geriatric” by definition. The reason for the current approach was that the access paths to 1 of the 2 geriatric treatment systems are very different and result in a different selection of patients. Meinck et al., for example, showed, with German routine data from the same time period, that patients receiving a geriatric early rehabilitative treatment (OPS 8–550 procedure) clearly had a higher rate of care need and a considerably lower survival rate than patients receiving sub-acute geriatric rehabilitation (14). Therefore, the direct comparison of patients who have received 1 of the 2 geriatric treatments has a high risk of residual confounding. The current study used a more systemic approach by comparing federal states that almost exclusively offered 1 of the 2 geriatric systems at the specific time the data were retrieved. Furthermore, the 3 federal states were situated close to each other, had a similar socioeconomic structure, and a similar capacity of geriatric beds, which was a good basis for comparison of the geriatric systems.
These data suggest that hip fracture patients from federal states with access to sub-acute geriatric rehabilitation had more favourable outcomes. Hip fractures and other fragility fractures are major causes of incident care need and disability, and not only of mortality. The results of the current study indicate that hip fracture treatment requires more considerations than just a perfect surgical treatment and a few days of postsurgical physiotherapy in order to reduce post-acute disability. However, the results of the outcome “nursing home admission” must be interpreted with caution, since an (impressive) reduction in nursing home admissions was observed only in Baden-Wuerttemberg, but not in Bavaria. Basically, a reduction in nursing home admissions of more than 20% would mean that many nursing home admissions could be prevented, or at least delayed. The costs of nursing home treatment include more than 20,000 € p.a. from the payer perspective and an equivalent amount for the patients and relatives.
A major issue in the ongoing debate in Germany has been that the costs of rehabilitation are covered by the healthcare funds, and the savings are made by other stakeholders, such as patients, long-term care plans and communities reducing their contribution to welfare plans for older people. This conflict of interest has led to a delayed reform of the regulatory process, ensuring access to geriatric rehabilitation in those states that have postponed the introduction of sub-acute geriatric rehabilitation.
The strengths of this study are the large number of included patients with fractures and the statistical competing risk approach for the primary outcomes “increase in care dependency” and “nursing home admission”, since mortality clearly influences the rate of the other primary outcome measures. Another strength is the selection of an appropriate time-window for this German historical natural experiment. To avoid bias in the analyses of rehospitalization, left truncated analyses were performed using one observation per person-day under risk.
Limitations
A limitation of the study is that information about the primary outcomes care dependency/care need and nursing home status was available only on a quarterly basis. This impaired precision, but did not bias the results. Other limitations of the study arise from the restricted information derivable from health claims data, such as missing information about why patients received no rehabilitation at all or about frailty, physical activity, or other lifestyle factors. In addition, the current study analysed only 3 federal states. The validity would clearly have been higher if more federal states with “pure” systems had been included. This study also only analysed persons insured by one German statutory health insurance company, which covers approximately one-third of the population. However, this may limit the representativity of the results for the whole of Germany. In addition, the historical approach may restrict the transferability of the results shown to the present time. Furthermore, the results may have been affected by other factors that were not adjusted for, such as the availability of social networks for the outcome “nursing home admission”.
It is the nature of the study to analyse associations that may be influenced by the specific structure of the German healthcare system. Hence, the generalizability of the study results to other countries is low. On the other hand, the specific structure of the German healthcare system may have been useful to analyse basic principles of geriatric rehabilitation. This study could be a blueprint for the analysis of different geriatric treatment models in Europe, by using other “historical natural experiments”. These data suggest that elderly and frail patients appear to benefit from supportive sub-acute rehabilitative care, which goes beyond appropriate acute care. Further interesting research questions would be whether this care has to be delivered in an inpatient setting or whether it may also be effective at home or in a nursing home, and if a combination of both geriatric treatment systems has additional value.
Conclusion
In conclusion, the potential health benefit of 2 geriatric rehabilitation systems was analysed by comparing the outcomes of geriatric patients with hip fracture between different federal states offering mainly 1 of the 2 geriatric rehabilitation systems. The risk of an increase in care dependency/care need and of rehospitalization was higher in the federal state that offered acute geriatric care than in the 2 federal states that offered sub-acute geriatric rehabilitation. However, the association with nursing home admission was inconsistent and no difference was found in mortality between the 2 geriatric healthcare systems.
The authors thank Christian Günster and Jürgen-Bernhard Adler from WIdO for their support in providing the data and Martin Rehm for running the statistical calculations and preparing tables and figures.
This work was supported by the German Federal Ministry of Education and Research within the project “Prevention and Rehabilitation of Osteoporotic Fractures in Disadvantaged Populations 2 (PROFinD2)” grant number 01EC1404E.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize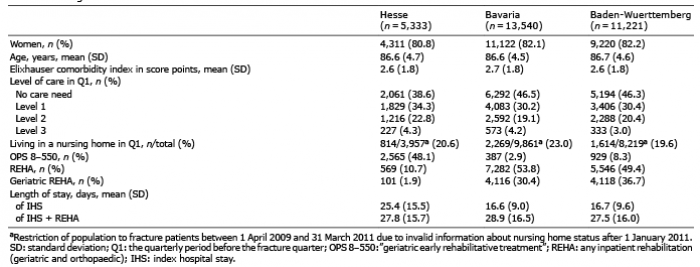 Click to show fullsize
Click to show fullsize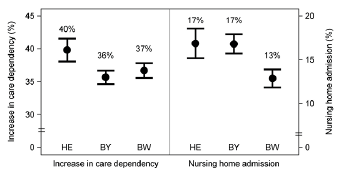 Click to show fullsize
Click to show fullsize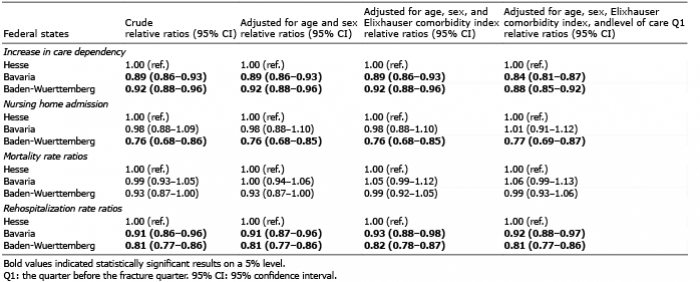 Click to show fullsize
Click to show fullsize